Sugar Coating the Kidneys
1
View details
A 68-year-old male presents to the clinic for a routine follow-up of his type 2 diabetes mellitus and hypertension. He reports feeling generally well, though he notes mild fatigue that has persisted for several months. He denies dysuria, hematuria, or changes in urinary frequency. His current medications include metformin 1000 mg twice daily, lisinopril 20 mg daily, and amlodipine 5 mg daily. He has a 20-pack-year smoking history but quit 10 years ago. Review of systems is otherwise negative for chest pain, shortness of breath, or lower extremity swelling.
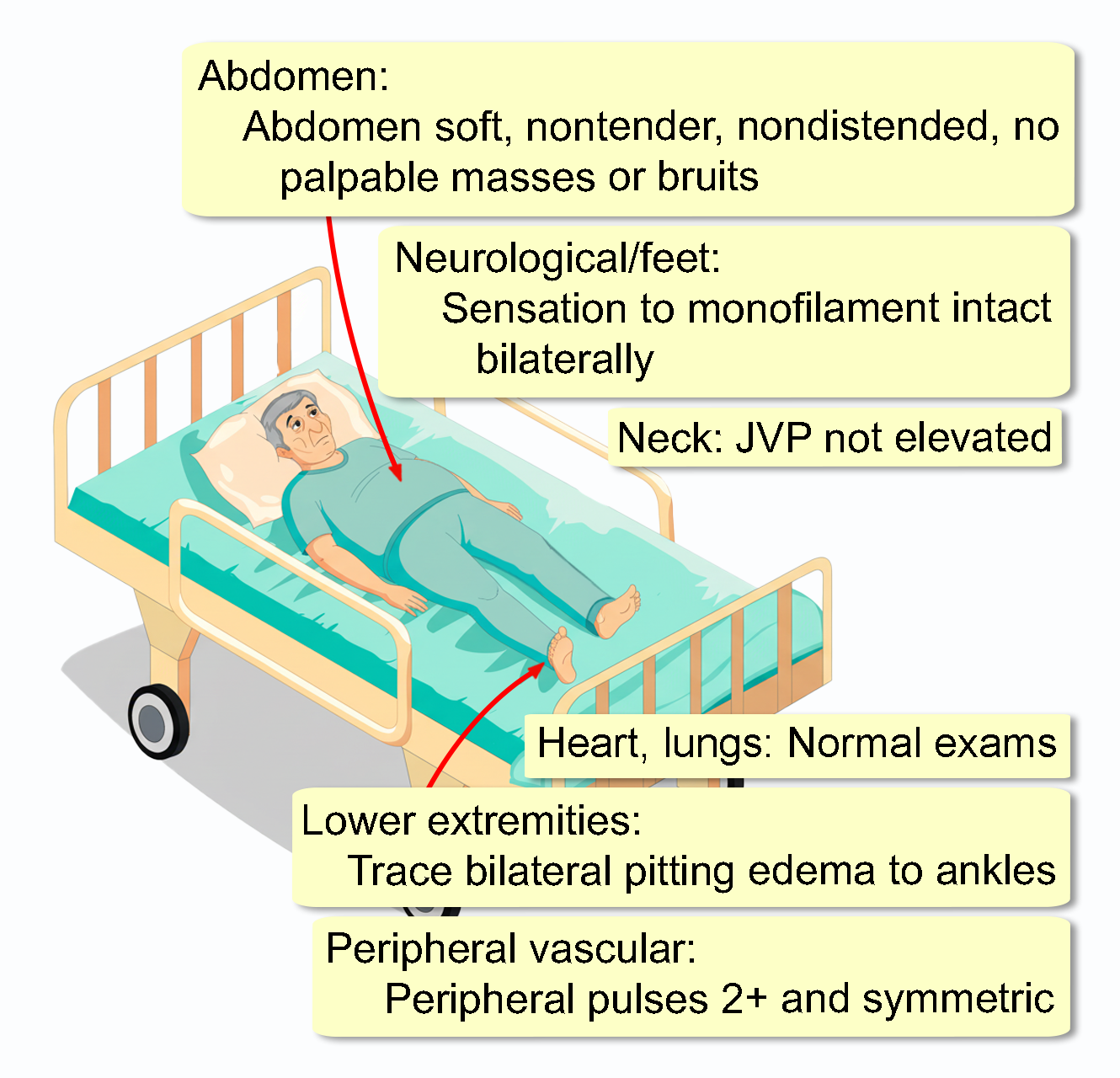
He appears comfortable and well-nourished. He is obese. His blood pressure is 142/86 mmHg with a heart rate of 76 bpm. He is afebrile with a respiratory rate of 14/min and an oxygen saturation of 98% on room air. His mucous membranes are moist.